Is sterilization more effective with wrapped or unwrapped equipment? How does wrapping equipment affect the autoclaving process?
In an autoclave there are many different cycles. There is a glass cycle, plastic cycle, wrapped and unwrapped cycle. You cannot, for example, run plastic in a glass cycle.
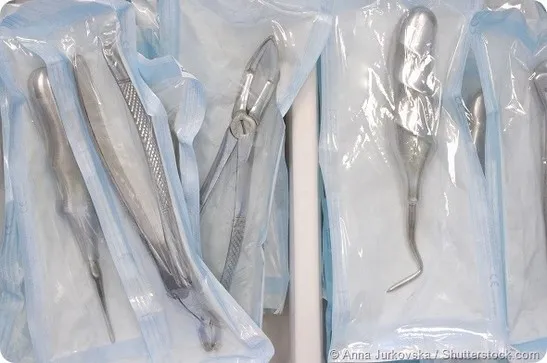
The equipment in the glass and plastics cycles are usually those left unwrapped, neither is better than the other, they simply serve different functions. A wrapped cycle, is where tools have been wrapped up and will remain wrapped until use.
That use could be days or weeks from now, but we will need those tools and we can’t wait until then to sterilize them, as they might otherwise spread disease. We also don’t want to sterilize them twice, once immediately after use and once before they are used again, as that is a waste of resources.
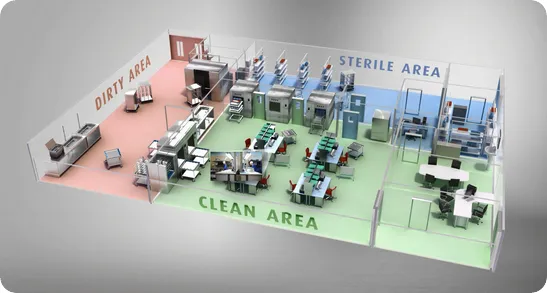
So a wrapped cycle allows you to sterilize the tools and the small wrapped environment that they are in, allowing us to know that they will remain sterile until they are needed.
On the other hand, an unwrapped cycle is for tools that are going to be used immediately, for example, in smaller medical environments like your dentist’s, they aren’t going to have hundreds of knives.
Instead maybe a couple of sets, which they may need to use repeatedly on different customers throughout the day. They can sterilize a set while taking care of a patient and use the newly sterilized set with the following patient.